

If you’re looking into outpatient treatment, you’re probably wondering how it will fit into your life — and fitting around your life is the whole point. Unlike inpatient or residential rehab, outpatient care doesn’t ask you to put everything on hold. You keep living at home, working, and showing up for the people who count on you, all while getting real, structured treatment. Below we walk through the three levels — PHP, IOP, and Supportive Outpatient — in plain numbers: hours per week, what a typical week looks like, how long each runs, and what insurance usually covers.
Last reviewed and updated June 2026.
- PHP (Partial Hospitalization): ~20–30 hrs/week, typically 2–4 weeks.
- IOP (Intensive Outpatient): ~9–12 hrs/week — 3 groups + 1 individual — typically 8–12 weeks.
- SOP (Supportive Outpatient): ~2–3 hrs/week, 3–12 months.
- Full continuum: about 4–6 months end to end; most direct-admit clients start at IOP, not PHP.
- What matters most: staying past 90 days — NIDA considers under 90 days “of limited effectiveness.”
The pattern to notice: as you move down the ladder, hours drop but the calendar gets longer. Intensity tapers; support stretches out.
PHP — Partial Hospitalization
PHP (ASAM Level 2.5) is the closest thing to inpatient care that still lets you sleep in your own bed. You’re at the center most of the day, most weekdays, doing the heavy lifting of early recovery — stabilizing, learning skills, and getting medical and psychiatric eyes on you regularly. A typical week is 4–5 group days at 5–6 hours each plus 1 individual session — think Monday–Friday, roughly 9:00 a.m.–2:30 p.m. Insurance reality: PHP is almost always pre-authorized and reviewed every 5–7 days, so you get the next few days at a time, then more if progress is documented.
IOP — Intensive Outpatient
IOP (ASAM Level 2.1) is where most outpatient clients spend the bulk of their time — and for many, where they start. It’s built to fit around a job, school, or family: 3 group sessions of about 3 hours each plus 1 individual session, often three weeknights (9 a.m.–noon or 6–9 p.m.). You get real structure and accountability without putting your whole life on hold. Insurers usually authorize IOP in chunks of about 10 program days, renewed on documented progress, and often support 6–8 weeks for clients who keep showing up.
SOP — Supportive Outpatient
Supportive Outpatient (ASAM Level 1.0, what some programs call standard or general outpatient) is the maintenance layer — the part that protects everything you built in PHP and IOP. It’s light on hours and long on the calendar: about 1 group session (90 minutes) plus 1 individual session a week, easy to keep even with a full schedule. Routine outpatient usually needs little or no prior authorization, though some commercial plans cap annual sessions and review periodically.
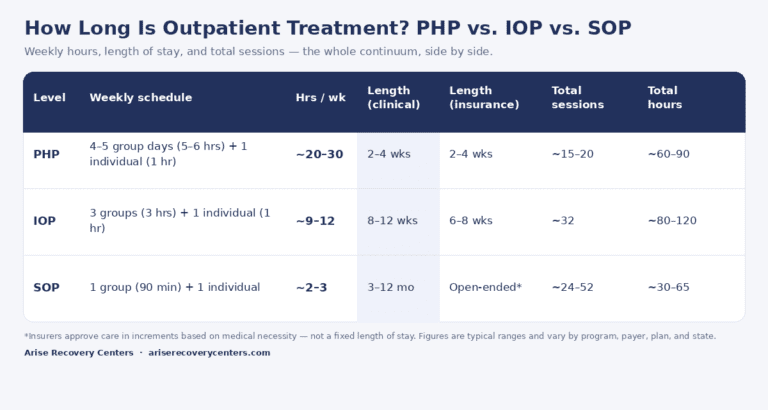
The whole picture, side by side
| Level | Weekly schedule | Hrs/wk | Length (clinical) | Length (insurance) | Total hours |
|---|---|---|---|---|---|
| PHP | 4–5 group days (5–6 hrs) + 1 individual | ~20–30 | 2–4 wks | 2–4 wks, in 5–10 day blocks | ~60–90 |
| IOP | 3 groups (3 hrs) + 1 individual | ~9–12 | 8–12 wks | 6–8 wks, ~10-day increments | ~80–120 |
| SOP | 1 group (90 min) + 1 individual | ~2–3 | 3–12 mo | Open-ended* | ~30–65 |
*Insurers don’t grant a “length of stay” up front — they approve increments and require concurrent review.
Where do people start? Two ways in
1. Step-down. You finish a higher level of care — medical detox, inpatient, or residential — and step down into PHP or IOP to keep your momentum. This is the classic continuum, and the safest route after a medically managed start.
2. Direct admission. Many people come straight to outpatient without any higher level first — especially those with mild-to-moderate use, a stable home, and work or school to protect. For these clients, IOP is the front door, with PHP for higher-acuity cases. Starting at SOP is rare.
In national SAMHSA data, Supportive Outpatient looks like the most common starting point — but that figure is inflated by long-term medication maintenance and court- or DUI-mandated counseling, not people choosing rehab. In real clinical practice, SOP is almost never where treatment begins — it’s the step-down tail.
The whole program, start to finish
Strung together, the continuum is designed to taper — high intensity early, lighter touch over time — and to span roughly 4 to 6 months from first day to last.
~3 weeks PHP + ~8 weeks IOP + ~12 weeks SOP ≈ 5–6 months and roughly 170–275 total hours of care — the typical path when stepping down from detox or residential, or entering with higher acuity.
~8–12 weeks IOP + ~12–24 weeks SOP ≈ 4–6 months and roughly 110–185 total hours. This is where most direct-admission clients live: start intensive, then taper into long-term support.
Hours on the calendar vs. results that last
Here’s where length stops being a scheduling question and becomes the single biggest predictor of success. The National Institute on Drug Abuse considers under 90 days of treatment “of limited effectiveness,” and one-year sobriety climbs steeply the longer someone stays — from roughly 15–30% after a 30-day stay to 55–70% past 90 days, and 70–85% with six or more months of care. The catch: about 30% drop out in the first month and more than half before three months — right before treatment starts to pay off. The goal of the whole continuum is to keep meaningful support in place long enough for new habits to hold.
Wondering what it would actually cost you? Run your plan through our Cost of Treatment calculator to see your out-of-pocket cost with insurance versus self-pay.
Frequently asked questions
PHP runs about 20–30 hours a week; IOP about 9–12 hours (three groups plus one individual session); Supportive Outpatient about 2–3 hours.
PHP typically 2–4 weeks, IOP 8–12 weeks, and SOP 3–12 months. Strung together, the full continuum usually spans about 4–6 months.
No. Most people who come straight to outpatient start at IOP. PHP is for higher-acuity cases or stepping down from detox, inpatient, or residential care.
Usually yes — IOP and SOP are built around work and school, with morning, evening, and telehealth options. PHP is more time-intensive and often pairs with short-term leave.
Most commercial plans, Medicare, Medicaid, and TRICARE cover medically necessary PHP, IOP, and outpatient care — approved in increments based on medical necessity. Verify your benefits to see your specific coverage.
Yes. NIDA considers under 90 days “of limited effectiveness.” One-year sobriety climbs from ~15–30% after 30 days to 55–70% past 90 days, and 70–85% with six-plus months of care.
Ready to take the first step?
We’ll check your benefits and help you find the right level of care — free, confidential, no obligation.