Skip to content
888-339-2747
Free Phone Consultation
HOME
ABOUT US
OUR STORY
WHY ARISE RECOVERY CENTERS?
OUR TEAM
LOCATIONS
TESTIMONIALS
BLOG
FAQS
CAREERS
OUTPATIENT DRUG REHAB
OUTPATIENT ALCOHOL REHAB
LEVELS OF CARE
OUTPATIENT REHAB
INPATIENT REHAB
HOUSTON
FORT WORTH
DALLAS
AUSTIN
DRUG & ALCOHOL DETOX
HOUSTON
DALLAS
AUSTIN
SOBER LIVING
HOUSTON
FORT WORTH
DALLAS
AUSTIN
ADDITIONAL SERVICES
INTENSIVE OUTPATIENT PROGRAM
SUPPORTIVE OUTPATIENT PROGRAM
FAMILY PROGRAM
EMDR THERAPY
TELEMEDICINE THERAPY
RELAPSE PREVENTION
AFTERCARE PLANNING
PARTIAL HOSPITALIZATION PROGRAM
EMPLOYER SERVICES
DRUG TESTING
MEDICAL FORMS
DFW LOCATIONS
ARLINGTON
DALLAS
FORT WORTH
MCKINNEY
SOUTHLAKE
ROCKWALL
AUSTIN LOCATIONS
SOUTH AUSTIN
NORTH AUSTIN
HOUSTON LOCATIONS
NORTH HOUSTON / CYPRESS
WEST HOUSTON / MEMORIAL
SUGAR LAND
THE WOODLANDS
SCHEDULE FREE CONSULTATION
VERIFY YOUR INSURANCE
PAY YOUR BILL
HOME
ABOUT US
OUR STORY
WHY ARISE RECOVERY CENTERS?
OUR TEAM
LOCATIONS
TESTIMONIALS
BLOG
FAQS
CAREERS
OUTPATIENT DRUG REHAB
OUTPATIENT ALCOHOL REHAB
LEVELS OF CARE
OUTPATIENT REHAB
INPATIENT REHAB
HOUSTON
FORT WORTH
DALLAS
AUSTIN
DRUG & ALCOHOL DETOX
HOUSTON
DALLAS
AUSTIN
SOBER LIVING
HOUSTON
FORT WORTH
DALLAS
AUSTIN
ADDITIONAL SERVICES
INTENSIVE OUTPATIENT PROGRAM
SUPPORTIVE OUTPATIENT PROGRAM
FAMILY PROGRAM
EMDR THERAPY
TELEMEDICINE THERAPY
RELAPSE PREVENTION
AFTERCARE PLANNING
PARTIAL HOSPITALIZATION PROGRAM
EMPLOYER SERVICES
DRUG TESTING
MEDICAL FORMS
DFW LOCATIONS
ARLINGTON
DALLAS
FORT WORTH
MCKINNEY
SOUTHLAKE
ROCKWALL
AUSTIN LOCATIONS
SOUTH AUSTIN
NORTH AUSTIN
HOUSTON LOCATIONS
NORTH HOUSTON / CYPRESS
WEST HOUSTON / MEMORIAL
SUGAR LAND
THE WOODLANDS
SCHEDULE FREE CONSULTATION
VERIFY YOUR INSURANCE
PAY YOUR BILL
HOME
ABOUT US
OUR STORY
WHY ARISE RECOVERY CENTERS?
OUR TEAM
LOCATIONS
BLOG
FAQS
CAREERS
DRUG REHAB
ALCOHOL REHAB
ADDITIONAL SERVICES
PARTIAL HOSPITALIZATION PROGRAM
INTENSIVE OUTPATIENT PROGRAM
SUPPORTIVE OUTPATIENT PROGRAM
FAMILY PROGRAM
EMDR THERAPY
TELEMEDICINE THERAPY
RELAPSE PREVENTION
AFTERCARE PLANNING
EMPLOYER SERVICES
DRUG TESTING
MEDICAL FORMS
VIRTUAL IOP (ONLINE)
REHAB RESOURCES & GUIDES
LEVELS OF CARE
OUTPATIENT REHAB
INPATIENT REHAB
HOUSTON
FORT WORTH
DALLAS
AUSTIN
DRUG & ALCOHOL DETOX
HOUSTON
DALLAS
AUSTIN
SOBER LIVING
HOUSTON
FORT WORTH
DALLAS
AUSTIN
TESTIMONIALS
LOCATIONS
ARLINGTON
DALLAS
FORT WORTH
MCKINNEY
ROCKWALL
SOUTHLAKE
NORTH HOUSTON / CYPRESS
WEST HOUSTON / MEMORIAL
SUGAR LAND
THE WOODLANDS
SOUTH AUSTIN
NORTH AUSTIN
PAY YOUR BILL
HOME
ABOUT US
OUR STORY
WHY ARISE RECOVERY CENTERS?
OUR TEAM
LOCATIONS
BLOG
FAQS
CAREERS
DRUG REHAB
ALCOHOL REHAB
ADDITIONAL SERVICES
PARTIAL HOSPITALIZATION PROGRAM
INTENSIVE OUTPATIENT PROGRAM
SUPPORTIVE OUTPATIENT PROGRAM
FAMILY PROGRAM
EMDR THERAPY
TELEMEDICINE THERAPY
RELAPSE PREVENTION
AFTERCARE PLANNING
EMPLOYER SERVICES
DRUG TESTING
MEDICAL FORMS
VIRTUAL IOP (ONLINE)
REHAB RESOURCES & GUIDES
LEVELS OF CARE
OUTPATIENT REHAB
INPATIENT REHAB
HOUSTON
FORT WORTH
DALLAS
AUSTIN
DRUG & ALCOHOL DETOX
HOUSTON
DALLAS
AUSTIN
SOBER LIVING
HOUSTON
FORT WORTH
DALLAS
AUSTIN
TESTIMONIALS
LOCATIONS
ARLINGTON
DALLAS
FORT WORTH
MCKINNEY
ROCKWALL
SOUTHLAKE
NORTH HOUSTON / CYPRESS
WEST HOUSTON / MEMORIAL
SUGAR LAND
THE WOODLANDS
SOUTH AUSTIN
NORTH AUSTIN
PAY YOUR BILL
Arise Recovery Centers Medical Forms
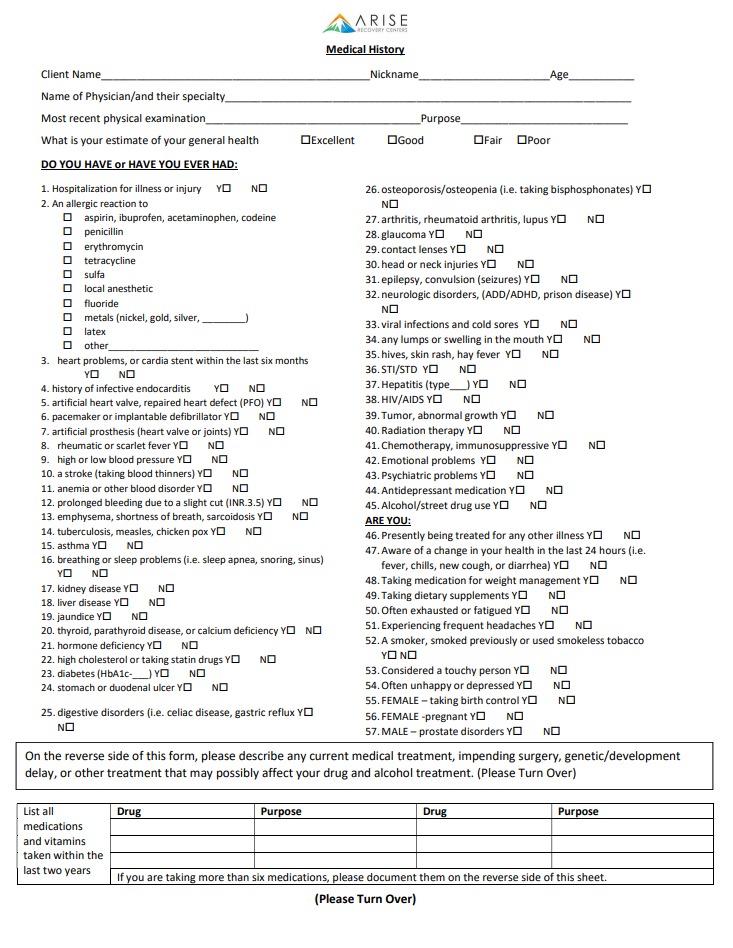
Medical History Form
PRINT & RETURN IN OFFICE
SUBMIT ONLINE
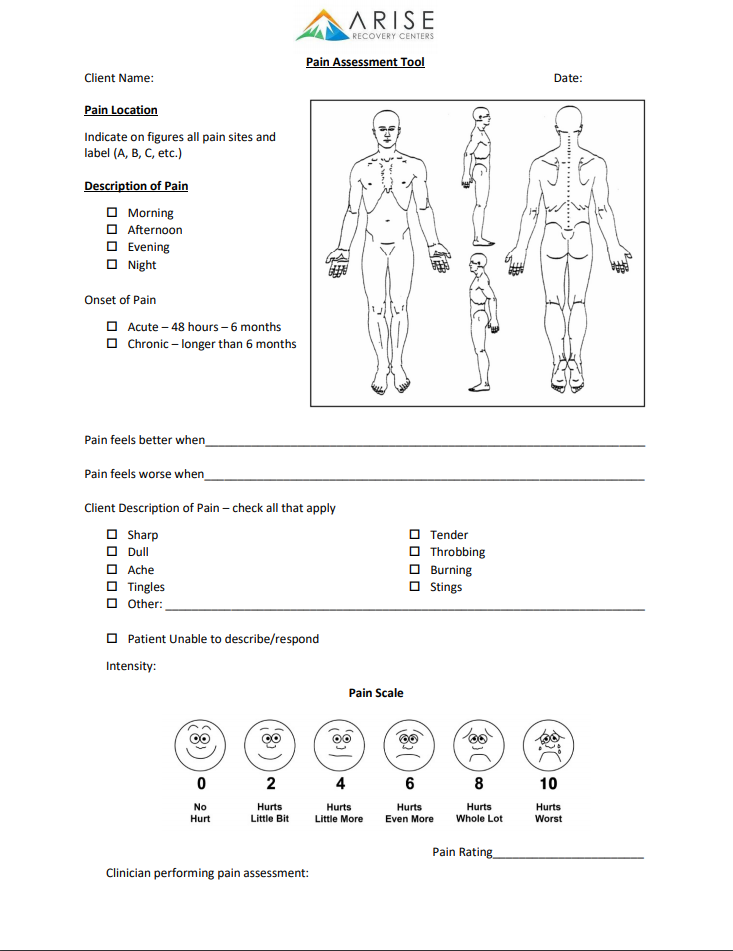
Pain Assessment Form
PRINT & RETURN IN OFFICE
SUBMIT ONLINE
Online Medical History Form
Patient Name
Nickname
Age
Name of Physician & Their Specialty
Most Recent Physical Examination
Purpose
Preferred Clinic Location
Select One
Dallas
Fort Worth
McKinney
Southlake
Insurance Policy Holder Name
Insurance Policy Holder Date of Birth
What is your estimate of your general health?
Excellent
Good
Fair
Poor
DO YOU HAVE or HAVE YOU EVER HAD:
1. Hospitalization for illness or injury?
Yes
No
2. An allergic reaction to:
aspirin
penicillin
erythromycin
tetracycline
sulfa
local anesthetic
fluoride
metals (nickel, gold, silver, other)
latex
other
3. Heart problems, or cardiac stent within the last six months?
Yes
No
4. History of infective endocarditis?
Yes
No
5. Artificial heart valve, repaired heart defect (PFO)?
Yes
No
6. Pacemaker or implantable defibrillator?
Yes
No
7. Artificial prosthesis (heart valve or joints)?
Yes
No
8. Rheumatic or scarlet fever?
Yes
No
9. High or low blood pressure?
Yes
No
10. A stroke (taking blood thinners)?
Yes
No
11. Anemia or other blood disorder?
Yes
No
12. Prolonged bleeding due to a slight cut (INR > 3.5)?
Yes
No
13. Emphysema, shortness of breath, sarcoidosis?
Yes
No
14. Tuberculosis, measles, chicken pox?
Yes
No
15. Asthma?
Yes
No
16. Breathing or sleep problems (i.e. sleep apnea, snoring, sinus)?
Yes
No
17. Kidney disease?
Yes
No
18. Liver disease?
Yes
No
19. Jaundice?
Yes
No
20. Thyroid, parathyroid disease, or calcium deficiency?
Yes
No
21. Hormone deficiency?
Yes
No
22. High cholesterol or taking statin drugs?
Yes
No
23. Diabetes (HbA1c=)?
Yes
No
24. Stomach or duodenal ulcer?
Yes
No
25. Digestive disorders (i.e. celiac disease, gastric reflux)?
Yes
No
26. Osteoporosis/osteopenia (i.e. taking bisphosphonates)?
Yes
No
27. Arthritis, rheumatoid arthritis, lupus?
Yes
No
28. Glaucoma?
Yes
No
29. Contact lenses?
Yes
No
30. Head or neck injuries?
Yes
No
31. Epilepsy, convulsions (seizures)?
Yes
No
32. Neurologic disorders (ADD/ADHD, prion disease)?
Yes
No
33. Viral infections and cold sores?
Yes
No
34. Any lumps or swelling in the mouth?
Yes
No
35. Hives, skin rash, hay fever?
Yes
No
36. STI / STD?
Yes
No
37. Hepatitis?
Yes
No
38. HIV / AIDS?
Yes
No
39. Tumor, abnormal growth?
Yes
No
40. Radiation therapy?
Yes
No
41. Chemotherapy, immunosuppressive?
Yes
No
42. Emotional problems?
Yes
No
43. Psychiatric treatment?
Yes
No
44. Antidepressant medication?
Yes
No
45. Alcohol / street drug use?
Yes
No
46. Presently being treated for any other illness?
Yes
No
47. Aware of a change in your health in the last 24 hours?
Yes
No
48. Taking medication for weight management (i.e. fen-phen)?
Yes
No
49. Taking dietary supplements?
Yes
No
50. Often exhausted or fatigued?
Yes
No
51. Experiencing frequent headaches?
Yes
No
52. A smoker, smoked previously or use smokeless tobacco?
Yes
No
53. Considered a touch person?
Yes
No
54. Often unhappy or depressed?
Yes
No
55. FEMALE - taking birth control pills?
Yes
No
56. FEMALE - pregnant?
Yes
No
57. MALE - prostate disorders?
Yes
No
Describe any current medical treatments:
Drug
Purpose
Drug
Purpose
Drug
Purpose
Drug
Purpose
SUBMIT
Online Pain Assessment Form
Patient Name
Admission #
Date
Pain Location
Head
Neck
Shoulder
Arm
Chest
Abdomen / Stomach
Pelvic
Thigh
Knee
Ankle
Foot
Pain is Worse
Morning
Afternoon
Evening
Night
Onset of Pain
Acute - 48 Hours - 6 Months
Chronic - Longer Than 6 Months
Pain Feels Better When...
Pain Feels Worse When...
Pain Description of Pain - Check All That Apply
Sharp
Dull
Ache
Tingles
Stings
Tender
Throbbing
Burning
Other
Unable to Describe / Respond
Pain Scale
No Pain
1-3 Mild
4-6 Moderate
7-10 Severe
Nurse Performing Pain Assessment
SUBMIT